SanJose Honduras
Dr Vega made her first trip to SanJose Honduras as a part of the Global Health at Family Medicine at The University of Rochester ,She has traveled to Honduras on seven occasions and is getting ready to travel again in may.
400 Children
Dr. Vega coordinates the dental program during her visits to Honduras. This includes the administration of a Fluoride program for 400 Children.
SanJose Honduras
Helping the people of San Jose was the best experience during my residency training. It continues to be one of the most rewarding experiences of my career.e
SanJose Honduras
“It is a completely different reality there, and having a hands-on role in improving the life of communities who are working toward sustainable development is so very deeply rewarding.”
Pediatrics Dentistry
How does tooth decay affect baby teeth?
Tooth decay in the primary (baby) teeth of young children is also called early childhood caries. Caries is another word for a cavity. It happens when the child’s teeth come into contact with sugary foods and drinks often and for long periods of time. These drinks include fruit juices, soda and other drinks with sugar.
Parents are often surprised to learn that tooth decay can begin as soon as a baby´s teeth come in, Usually, by age six months. Decay in baby teeth can cause pain, and the infection can spread. If decay is not treated, it can destroy the baby teeth.
Tooth decay can also have an effect on a child´s general health. If a child has tooth pain, she may have trouble eating. The child may not get enough vitamins and minerals to grow up healthy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Why are baby teeth important?
Babe teeth hold space in the jaw for the adult teeth. If a baby tooth is lost too early, the teeth
Beside it may drift into the empty space.
When it´s time for the adult teeth to come in, there may not be enough room for them. This may cause adult teeth to be crowded and crooked. Crooked teeth may be hard to keep clean.
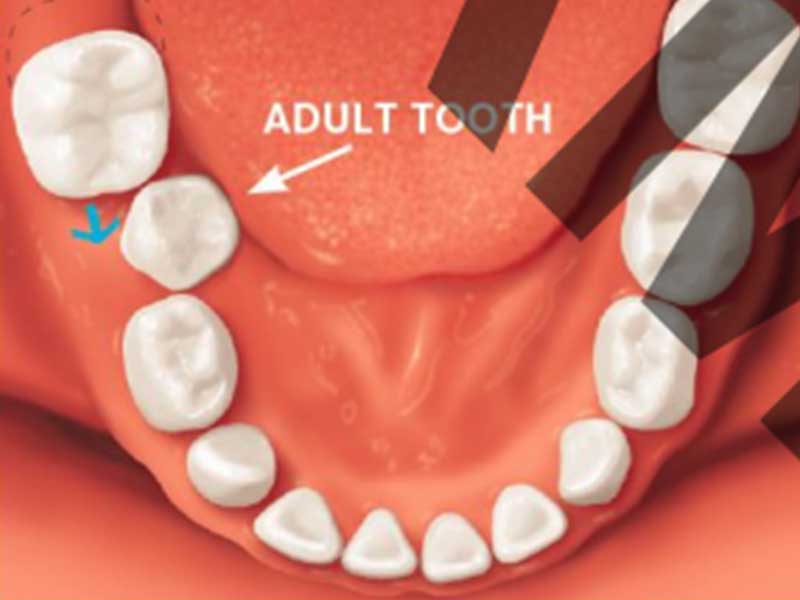
If a baby tooth is lost too early, the teeth beside it may drift into the empty space.
If a child´s baby teeth are healthy, it is more likely his adult teeth will be healthy too. Children who have decay in their baby teeth are more likely to have decay in their adult teeth.
Decayed and crooked teeth also can affect your child´s self-esteem. Tooth decay is not only unhealthy, it also looks bad. It also looks bad. If your child has tooth decay he may feel bad about his smile. On the other hand, a nice-looking smile can give your child confidence at school.
How to keep your child’s teeth healthy
Children learn healthy habits from their parent and caregivers. You can start good habits if you Clean your child´s teeth every day, feed your child a healthy diet and take her to the dentist regularly.
Clean your child’s teeth at home
* Wipe the baby’s gums with a clean, wet gauze pad or washcloth after each feeding, beforesleep. This removes bits of food that can harm teeth that are starting to come in. It also helps the child get used to having his mouth cleaned.
* As soon as the first tooth appears, start brushing your baby’s teeth twice a day (morning and night). Use a soft-bristled, child-sized toothbrush and a fluoride toothpaste. Until the child is three years old, use no more than a smear or grain-of-rice-sized amount of fluoride toothpaste. For children three to six years old, use no more than a pea-sized amount of fluoride toothpaste. * The American Dental Association recommends that you brush your child’s teeth until she is at least six years old. When your child is old enough to do the brushing, watch to make sure she is not "rushing the brushing." Children should be taught to spit out toothpaste, not swallow it.
For children under three years old

For children three to six years old

Bottles, pacifiers and breastfeeding
• Infants should finish their bedtime or naptime bottle before going to bed.
• After your child’s first tooth comes in, he should not be allowed to breastfeed constantly or fall
asleep while breastfeeding.
• Infants should not be put to bed or allowed to fall asleep with a bottle that contains milk, formula,
fruit juices, or any liquids with sugar. Even watered-down drinks can damage teeth.
• If your child uses a pacifier, don’t dip it in sugar or honey. Also, do not put it in your mouth before
giving it to the child. Decay-causing bacteria in your mouth can be passed to your baby.
• A bottle should not be used as a pacifier. Frequent sips of sugary liquids can cause tooth decay.
Training ("sippy") cups
• To lower the risk of tooth decay, try to get your child to drink from a cup by her first birthday.
• Do not let your baby constantly sip on liquids with sugar (including juice drinks). Offer these liquids
only at mealtimes. Keep the cup out of reach while the child is in a car or stroller. If your child is
thirsty between snacks or meals, offer water in the cup.
• Training cups should be used for only a short time. Once your child has learned how to sip, the
training cup is no longer needed and should be set aside.
A healthy diet builds strong teeth
• Limit between-meal snacks.
• Avoid using sweet foods and drinks to reward your child.
• If your child eats sweets, make sure it is with a meal.
• Infants and young children should have a healthy diet. Information can be found at
www.choosemyplate.gov
First Dental Visit
• Talk to your dentist about planning the child’s first dental visit. It’s helpful to have the first visit
after the baby's first tooth appears but no later than the first birthday. This first visit is a “well-baby
checkup” for your child’s teeth.
• At this visit, the dentist can check for decay and other problems. He or she can show you how to
properly clean your child’s teeth.
• Also, the dentist may offer advice on your child’s diet, pacifier use, and oral care products for your
family. He or she can tell you how to prevent injuries to your child’s teeth and mouth and what to do
in case of a dental emergency.
• Also, the dentist may offer advice on your child’s diet, pacifier use, and oral care products for your
family. He or she can tell you how to prevent injuries to your child’s teeth and mouth and what to do
in case of a dental emergency.
• Children should get the ideal level of fluoride to help prevent tooth decay. Ask your child’s dentist
about how your child can get the right amount of fluoride.
Chairside Guide: Silver Diamine Fluoride in the Management of Dental Caries Lesions
Dental caries affects about one out of four children aged 2-5 years.1 Silver diamine fluoride (SDF), recently approved for use in the United States, has been shown to be efficacious in arresting caries lesions.2,3 It is a valuable therapy which may be included as part of a caries management plan for patients. Caries lesions treated with SDF usually turn black and hard. Stopping the caries process in all targeted lesions may take several applications of SDF, and reapplication may be necessary to sustain arrest.
Active cavitated caries lesions before application of SDF

SDF-treated lesions with temporary gingival staining

Case selection for application of silver diamine fluoride Patients who may benefit from SDF include those:
• With high caries risk who have active cavitated caries
lesions in anterior or posterior teeth;
• Presenting with behavioral or medical management challenges
and cavitated caries lesions;
• With multiple cavitated caries lesions that may not all
be treated in one visit;
• With dental caries lesions that are difficult to treat; and
• Without access to or with difficulty accessing dental care.
Criteria for tooth selection include:
• No clinical signs of pulpal inflammation or reports of
unsolicited/spontaneous pain.
• Cavitated caries lesions that are not encroaching on the
pulp. If possible, radiographs should be taken to assess
depth of caries lesions.
• Cavitated caries lesions on any surface as long as they are
accessible with a brush for applying SDF. (Orthodontic
separators may be used to help gain access to proximal
lesions.)
SDF can be used prior to restoration placement and as part
of caries control therapy.4 Informed consent, particularly highlighting
expected staining of treated lesions, potential staining
of skin and clothes, and need for reapplication for disease
control, is recommended.
• Remove gross debris from cavitation to allow better SDF
contact with denatured dentin.
• Carious dentin excavation prior to SDF application is not
necessary. As excavation may reduce proportion of arrested
caries lesions that become black, it may be considered for
esthetic purposes.
• A protective coating may be applied to the lips and skin
to prevent a temporary henna-appearing tattoo that can
occur if soft tissues come into contact with SDF.
• Isolate areas to be treated with cotton rolls or other isolation
methods. If applying cocoa butter or any other product
to protect surrounding gingival tissues, use care to not
inadvertently coat the surfaces of the caries lesions.
• Caution should be taken when applying SDF on primary
teeth adjacent to permanent anterior teeth that may have
non-cavitated (white spot) lesions to avoid inadvertent
staining.
• Careful application with a microbrush should be adequate
to prevent intraoral and extraoral soft tissue exposure. No
more than one drop of SDF should be used for the entire
appointment.
• Dry lesion with gentle flow of compressed air.
• Bend micro sponge brush. Dip brush into SDF and dab
on the side of the plastic dappen dish to remove excess
liquid before application. Apply SDF directly to only the
affected tooth surface. Remove excess SDF with gauze,
cotton roll, or cotton pellet to minimize systemic absorption.
• Application time should be at least one minute if possible.
(Application time likely will be shorter in very young and
difficult to manage patients. When using shorter application
periods, monitor carefully at post-op and re-care to
evaluate arrest and consider re-application.)
• Apply gentle flow of compressed air until medicament is
dry. Try to keep isolated for as long as three minutes.
• The entire dentition may be treated after SDF treatment
with five percent sodium fluoride varnish to help prevent
caries on the teeth and sites not treated with SDF.
Follow-up
Estimations of SDF effectiveness in arresting dental caries lesions range from 47 to 90 percent with one-time application depending on size of the cavity and tooth location.4-7 Anterior teeth have higher rates of arrest than posterior teeth.5 Therefore, follow-up for evaluation of caries arrest is advisable.2-3
• Follow-up at 2-4 weeks after initial treatment to check
the arrest of the lesions treated.
• Reapplication of SDF may be indicated if the treated
lesions do not appear arrested (dark and hard). Additional
SDF can be applied at recall appointments as
needed, based on the color and hardness of the lesion
or evidence of lesion progression.
• Caries lesions can be restored after treatment with SDF.
• When lesions are not restored after SDF therapy, biannual
re-application shows increased caries arrest rate
versus a single application.
Reference
1. Dye BA, Thornton-Evans G, Li X, Iafolla TJ. Dental caries and sealant prevalence in children and adolescents in the United States, 2011–2012. NCHS data brief, no 191. Hyattsville, Md.: National Center for Health Statistics. 2015. Available at: “https://www.cdc.gov/nchs/ products/databriefs/db191.htm”. Accessed September 6, 2017. (Archived in WebCite® at: “http://www.webcita tion.org/6tX0D6qO1”)
2. Gao SS, Zhang S, Mei ML, Lo EC, Chu CH. Caries remineralisation and arresting effect in children by professionally applied fluoride treatment – A systematic review. BMC Oral Health 2016;16:12.
3. Duangthip D, Jiang M, Chu CH, Lo EC. Restorative approaches to treat dentin caries in preschool children: Systematic review. Eur J Paediatr Dent 2016;17(2): 113-21.
4. Crystal YO, Niederman R. Silver diamine fluoride treatment considerations in children’s caries management: Brief communication and commentary. Pediatr Dent 2016;38(7):466-71.
5. Llodra JC, Rodriguez A, Ferrer B, Menardia V, Ramos T, Morato M. Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of schoolchildren: 36-month clinical trial. J Dent Res 2005;84(8):721-4.
6. Zhi QH, Lo ECM, Lin HC. Randomized clinical trial on effectiveness of silver diamine fluoride and glass ionomer in arresting dentine caries in preschool children. J Dent 2012;40(11):962-7.
7. Duangthip D, Jiang M, Chu CH, Lo EC. Restorative approaches to treat dentin caries in preschool children: Systematic review. Eur J Paediatr Dent 2016;17(2): 113-21.
© 2019. All Rights Reserved. Designe by Pedro Pablo Vega Guerrero